
Shining a bright light on extraordinary research talent in RI
Translational research grants made to Brown scientists to develop new genetic models to combat ALS and to apply acoustic analysis to infant cries to decipher and diagnosis withdrawal symptoms in babies
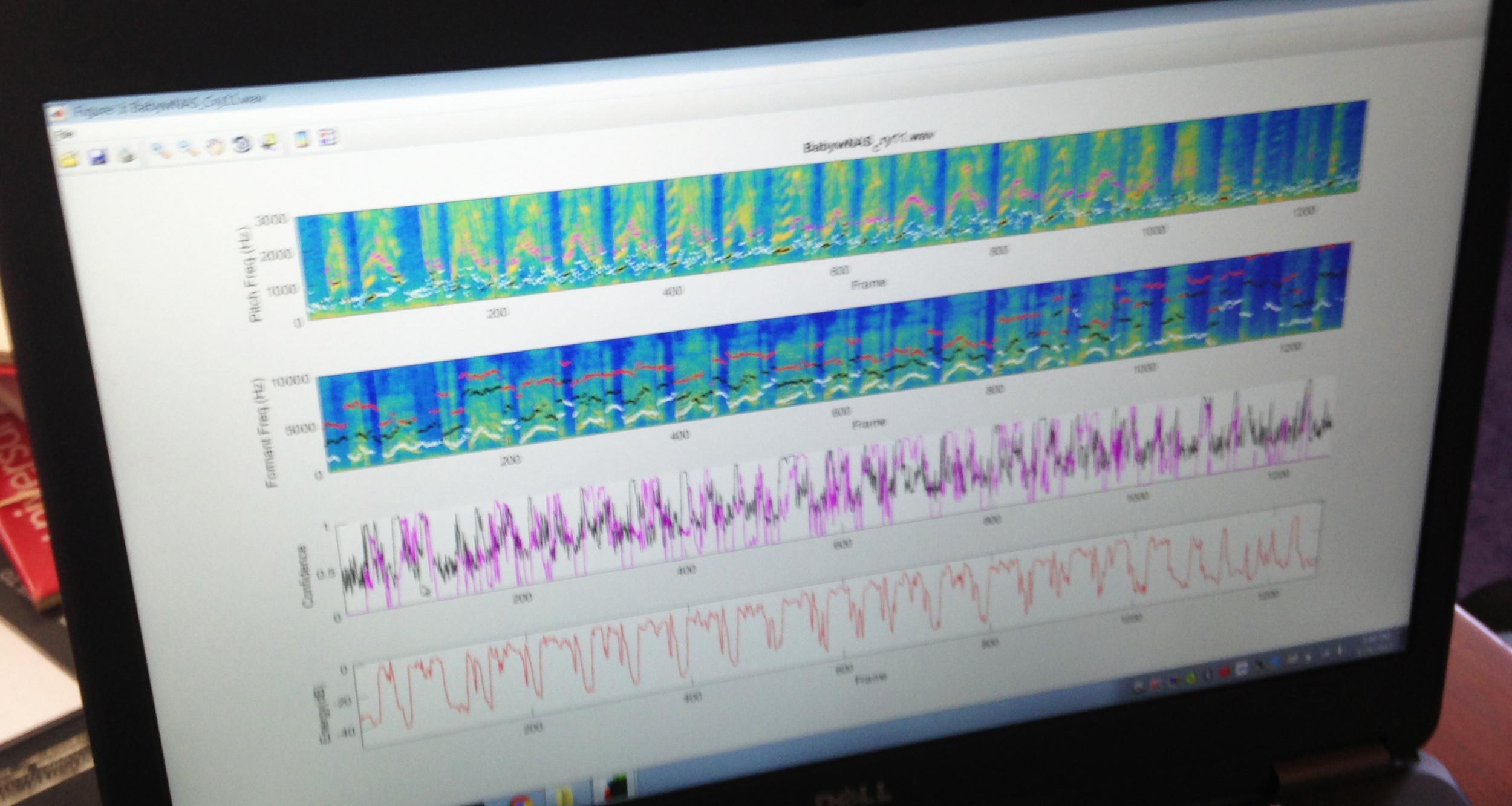
The acoustical analysis of a cry from an infant with Neonatal Abstinence Syndrome.
Stephen Sheinkopf, left, who is co-director of the R.I. Consortium for Autism Research and Treatment, and Steve Barry Lester, director of the Brown Center for the Study of Children at Risk.
PROVIDENCE – The distance between the research laboratory and the commercial market is an intangible space, often hard to measure. It is even harder to predict how long the journey may take or what the best roadmap will be to follow.
Two different but significant events occurred in the last two weeks, seeking to improve the odds of success on that journey within the biomedical and life sciences innovation ecosystem in Rhode Island.
On April 26, MedMates held its first annual Life Sciences Expo at the Omni Hotel in Providence, a confluence of entrepreneurs, scientists, startup firms, investors and policymakers, with more than 300 in attendance. The intent of the Expo was to showcase the state’s emerging biomedical innovation industry sector in Rhode Island, to further the connections within the cluster, and to attract new companies and investors to Rhode Island. [See link to ConvergenceRI story below.]
A week earlier, the new Biomedical Innovation Fund at Brown University announced its first two grants to accelerate the commercialization of technologies – one for diagnosing drug dependence in newborns and a second for the potential discovery of anti-ALS medicines, according to the news release by Brown.
The grants, each for $100,000, are an integral part of the initiative launched by Dr. Jack Elias, the dean of medicine and biologic sciences as a way to enhance Brown’s approach to translational research, working in partnership with the Technology Venture Office at Brown.
No longer lost in translation
The new translational grants are one of a number of initiatives now underway in Rhode Island, promoting efforts to connect research with the marketplace.
In February, the first two of six collaborative research awards for pilot projects planned for 2017 were announced as part of the five-year, $19.5 million Institutional Development Award from the National Institute of General Medical Sciences, a division of the National Institutes of Health. [See link to ConvergenceRI story, “And the winner is: Rhode Island and its innovation ecosystem.]
The new research program, known as the Advance-Clinical and Translational Research program, or Advance-CTR, addressed what Dr. Jim Padbury, the principal investigator, called “an unmet need for clinical translational research” in Rhode Island.
Earlier, in July of 2016, an MOU was signed establishing the first research partnership ever launched between a private drug discovery firm and the University of Rhode Island and its George and Anne Ryan Institute for Neuroscience, heralding a new era of public private collaboration in Rhode Island.
MindImmune Therapeutics, Inc., backed by an initial $500,000 in equity seed funding by the Slater Technology Fund, is targeting the development of first-in-class drugs to treat diseases of the central nervous system, including neurodegenerative afflictions such as Alzheimer’s and Huntington’s diseases.
The latest translational research grants through Brown offer a glimpse into the cutting-edge, world-class science being conducted here in Rhode Island, often under the radar screen.
Unlocking the genetic secrets of ALS
The research lab of Robert Reenan, professor of Biology at Brown, has engineered ALS-causing genetic mutations in fruit flies, or Drosophila. Reenan and his team have used that research to discover further mutations in what is known as a “suppressor gene” that mitigates the harmful effects of the disease.
The goal is to search for “small molecule” compounds that can pharmacologically achieve similarly beneficial effects in the ALS flies.
“These suppressor mutations identify a class of conserved human gene counterparts as potential drug targets of relevance in neurodegenerative disorders, such as ALS and dementia,” Reenan wrote in his application for the grant.
The work seeks to engineer fruit fly-expressing proteins from human gene counterparts in order to identify potential drug targets.
A new diagnostic syntax for infant cries
The second $100,000 translational research awards from the new Biomedical Innovation Fund at Brown University is focused on developing a diagnostic tool, analyzing the cries of babies, to make a more systemic and reliable diagnosis of Neonatal Abstinence Syndrome – the withdrawal symptoms when babies are born to mothers with an opioid addiction, an increasingly common condition among newborns.
The Brown research scientists involved with the project have built a sophisticated acoustic system and database to track and analyze the cries of infants. The grant will be used to develop a proof-of-concept project that seeks to attract potential investors in the development of an automated, hand-held, iPhone-like device.
ConvergenceRI met recently with Barry Lester, director of the Brown Center for the Study of Children at Risk, and Stephen Sheinkopf, who is co-director of the R.I. Consortium for Autism Research and Treatment, to talk about the new diagnostic tool and its potential applications for other kinds of conditions for children at risk.
[The work of Lester and his team will soon receive national exposure in an upcoming story in The New York Times Magazine.]
Here is the ConvergenceRI interview with Lester, as he explained the genesis of the science behind acoustic analysis of infants’ cries.
ConvergenceRI: I am fascinated by your work in analyzing infants’ cries. Are you still learning new things? Is there a sense of revelation? Is it like being a jazz musician and hearing a new riff?
LESTER: [laughing] I’ve never thought of it that way. I got into this in 1970. I was working in Guatemala, on a research study of malnourished children, jointly funded by the NIH and the World Health Organization.
These babies, when they cried, I had never heard anything like it. It was unusual. I knew that there was literature, a very, very primordial literature, on quote unquote “abnormal” baby cries.
I knew that there was some work that had been done in Sweden and Finland. [Lester gets up, searching his bookcases, and finds a published study.]
For example, this study was published in 1968; what they have in here are the cries of all different kinds of normal and abnormal babies. They were analyzed on something called the sound spectrograph.
It was a mechanical device, a rotating drum with a magnetic strip around it, with filters that pressed up against it. And when there was sound energy, it would leave these marks. These marks are acoustic measures [showing an photographic image from the published study].
This is the cycles per second, or Hertz [Hz]. This lower line is the fundamental frequency, or voice pitch. This baby cries, takes a breath, cries.
What they were doing was looking at different kinds of cries and trying to characterize them. Some of this is ridiculous – a “pleasure cry” doesn’t exactly make sense.
But the kind of revelation, and what became important about this [work], is when they started looking at the cries of babies that were abnormal.
Cri du chat, it’s a genetic anomaly [showing one of the illustrations in the study]. Cri du chat is French for cry of the cat. It’s actually similar to Down syndrome. The cry is so distinctive that when a baby is born [with this genetic disorder] and you hear the cry [Lester snaps his fingers], you don’t even need to do the genetic analysis, they do it anyway, but you know right away.
A normal baby’s cry is four or five hundred Hz cycles per second; this kid’s cry is a thousand. It’s extremely high pitched. And pitch doesn’t even characterize it. It’s hollow sounding; it still sends chills down my spine when I hear it.
This is really crude technology; this is 1968 before computers, this is “caveman” technology.
But, what it is showing is that when babies have brain damage, one of the main things you see is in changes in cry. Primarily, the thing that’s most obvious is this incredible high pitch.
ConvergenceRI: What the work seems to have done is to open up the potential to develop an acoustical detection system to better understand what an infant’s cry means.
LESTER: The real clue here, at least to me, was that the cry is telling you something about the integrity of the nervous system, a potential marker for CNS [central nervous system] involvement.
You can have a whole range of CNS involvement – meningitis or asphyxia.
We deal a lot with the universe of what we call infants at risk: babies who are at risk because of some condition. It could be malnutrition, it could be prematurity, it could be prenatal drug exposure. All these are quote unquote “at-risk” kids.
We know that some percentage [of at-risk babies] are going to have some kind of problem later on [in life].
So, if the cry is a window into the brain, then it is possible that the cry can be an early warning sign. The cry is telling you that there’s something going on here, that there is some kind of potential brain involvement, so that you can then differentiate.
I have these preemies, and their cries are normal; and I have these preemies, and their cries are higher pitched, or they have other characteristics. Does that mean that the ones with the higher pitched cries are more likely to have learning problems down the pipe?
That’s what kind of set me off, not just [identifying] Cri du chat, or asphyxia, but [recognizing] there were huge populations of kids at risk. You don’t need a cry to tell you that a baby has asphyxia. But, you may need a cry [to detemine] if a preemie is OK, or not OK.
If you can identify those who are highest risk, and then hone in on them, and develop whatever interventions and treatments [are needed].
ConvergenceRI: What happened following your work in Guatemala?
LESTER: I recorded the cries [of malnourished infants] when I was in Guatemala. Two years later, I came back to the States, got into a lab at Yale, where they were still using this “caveman” technology.
I analyzed the cries, how they were different, and that was published.
I then wound up doing a post-doctoral fellowship at Harvard, where I got involved with some people at MIT. This was in the late 1970s, computer systems were around, and we developed the first automated computerized acoustic analysis system.
Working with tape recordings, it would automatically read in the cry, download it, digitize it, and the computer would analyze all kinds of acoustic characteristics, not just pitch.
ConvergenceRI: What came next?
LESTER: We did a study [looking at whether] a cry might be characteristic of sudden infant death syndrome. We conducted a study of 22,000 babies at 11 hospitals across the country, looking at two specific cry features [to see if they] were diagnostic. It turns out, they weren’t. It was a close but no cigar situation. We identified two, but there was a third [characteristic] that was really necessary, but because it wasn’t hypothesized, you couldn’t turn it into a diagnostic tool.
Then I came down to Brown in 1985. A couple of years ago, we got an NIH grant to develop a whole new acoustical cry analysis system.
ConvergenceRI: Fast forward to where you are today. There are profound changes in the technology and in the accuracy of the sounds you’re able to capture. You have the capability to identify neonatal abstinence syndrome from the cries of infants. What is your hypothesis, moving forward?
LESTER: Within the work that we’re doing, we are introducing a new terminology, a new way to think about an actual acoustic cry signature for a specific syndrome.
That’s the work that we are doing. Yes, maybe pitch is involved with NAS. But is there something that is unique, a cry signature that is specific only to NAS, one that distinguishes it from not only normal babies, but from other at risk populations?
And, if there is, it opens the door for saying, if NAS has this unique signature, do other conditions have a unique signature, also?
ConvergenceRI: What are some of the other possibilities, in terms of conditions, that you would consider exploring as having potential cry signatures?
LESTER: Do you mean specific cry characteristics?
ConvergenceRI: Yes and no. For instance, something like toxic stress, with the ability to make diagnoses based upon cry signatures, with an early opportunity for intervention.
LESTER: When you say toxic stress, tell me what you’re thinking.
ConvergenceRI: More than just adverse childhood events, including things such as lead poisoning, conditions where toxicants are involved beyond heavy metal, such as environmental exposures, including PCBs, where the injury to the brain may not be cured by good social work.
LESTER: One of my big passions is epigenetics. And, part of my fascination with epigenetics is because while genotype is fixed, gene expression is not.
You can change gene expression, you can change the molecular basis of behavior.
Because of the incredible elasticity and rewiring of the brain, it means you can now think about treatments and interventions that are based on epigenetic understandings that can change gene expression and then change behavior.
If you take a peek at our website, it lists all the projects that are going on here. No matter what goes on, in research or seeing patients, we do epigenetics.
We have the largest autism [autism spectral disorder] outpatient clinic in Rhode Island as well as Southeastern Massachusetts.
Every single ASD patient that walks through our doors, we do cheek swabs.
ConvergenceRI: Does your work also involve research into toxicants, such as PCBs or mercury or chemicals such as PFOAs?
LESTER: We are part of an NIH program, called ECHO. Have you heard about that?
ECHO is a national study, it has 35 pediatric cohorts, and we’re one of the 35.
ECHO is all about everything you just mentioned, and then some – all the heavy metals, all the chemical exposures, everything.
It is an NIH-wide initiative. It’s a remarkable study. It’s being touted like the Framingham study. It is supposed to be the definitive study in child development. It’s going to go for seven years. It started in September; we’re in our first year.
Here’s the concept, which is really hard for some people to wrap their heads around. The idea is that you take these 35 cohorts, including all different kinds of kids, you can have preemies, you can have ASD.
To compete to participate in ECHO, the one thing you have to have is be an ongoing longitudinal pediatric cohort.
You collect whatever data the particular cohort is collected as part of a regular NIH-funded study, but then, you also collect a common set of environmental exposures.
We’re doing toenails and hair and teeth.
You do all that, you put all these cohorts together, the sample size is 50,000 kids, all different ages, all different populations, and put them all together, there’s a lot of noise in that system.
Are there environmental exposure signals that you detect that rise above the noise?
It’s an amazing initiative.
ConvergenceRI: Will you be able to apply your acoustical sound analysis system to try and decipher some of that “noise?”
LESTER: Our piece of ECHO, our cohort is premature infants. We have 620 that were born less than 30 weeks gestation.
These are kids who are most likely to be seriously impaired by two years of age; 30-35 percent will have serious impairments by two years of age.
What we’re trying to figure out is how early can we identify these babies, so that we can develop treatments and potential preventions, hopefully by the time they are discharged from the NICU, in order to reduce the magnitude of the deficits or prevent them in the first place.
How do we do that? There are three elements: one is cry, two is neuro-behavior, and three is epigenetics.
We have this neuro-behavioral exam that we developed [a while] ago for the NIH. It is a 15-minute exam. It is the industry standard for looking at neuro-behavior in high-risk infants. It has long-term predictive capability.
When you do the exam, one of the things that is really important is crying.
Part of the analysis of neuro-behavior is whether the baby is in good enough shape to be cry. You also want to know if they are competent enough to attempt to self-soothe or to be soothed, or are they totally out of control, which is your NAS kid – zero to 60 in 2.2 seconds. They are screaming and they are virtually inconsolable.
We record the cry during the exam, we run the cry through the acoustics, and we get epigenetics.
We do this at discharge [from the NICU] and then we see the kids at ages two, three, four, five, six and seven.
We are going to be looking at the epigenetics, not only at discharge, but at each of these ages.
The hypothesis is: can you develop a cumulative algorithm, a risk model, where you can say, if you have x cry characteristics, neuro-behaviors plus epigenetics, how well can I predict which of these kids are going to be impaired by age two? And can I do it with a sufficient degree of accuracy?
And, can I figure out which ones are most likely to be impaired and then develop specific treatments and interventions for them?




