
An action plan to redefine health, equity and community in Rhode Island
A new placed-based initiative, called Health Equity Zones, promises to put health back into health care, at the community level
Ana Novais, the executive director of the Division of Community, Family Health and Equity at the R.I. Department of Health, is coordinating the new initiative to create 11 Health Equity Zones, one in each county in Rhode Island.
Ana Novais, the executive director of the division of Community, Family Health and Equity at the R.I. Department of Health, in front of a map of Rhode Island showing where the 11 Health Equity Zones will be located.
PROVIDENCE – Ana Novais, the executive director of the Division of Community, Family Health and Equity at the R.I. Department of Health, has put together a remarkable initiative, one of the first of its kind in the nation, one that creates a unified theory of health, and translates that into collaborative endeavors at the community level.
Novais, with $2.15 million in federal funding from the Centers for Disease Control and Prevention, has put together a plan of action to improve the health of communities in Rhode Island.
The focus of the new initiative is about health, not health care, as Novais explained in an in-depth interview last week with ConvergenceRI.
The vision is to improve the conditions that cause poor health; it’s not about funding emergency services to perform rescues.
The overarching goal is to create a sustainable model based on population health as defined by community needs and relationships, not by medical models or metrics.
The basics of the program were shared in the recent news release: $2.15 million has been awarded to create 11 Health Equity Zones, including one in every county in Rhode Island, in the next three years.
As the news release detailed, the Health Equity Zones are charged with developing place-based strategies to reduce and manage chronic diseases, promote healthy lifestyles, assure healthy child development, and create environments where healthy choices are easier to make.
But, given the form that news releases must take, much of the context of the story and the ongoing narrative was missing.
The new initiative is actually the second-phase of work undertaken by earlier grants under the Centers for Health, Equity and Wellness program, or CHEW, targeted at neighborhood interventions, awarded to single community agencies. [See links below to articles in ConvergenceRI about the earlier CHEW programs.]
The news release diligently reported that the awards were given to 11 lead organizations representing a series of collaborations. They included: the city of Providence Healthy Communities’ office; the Olneyville Housing Corporation; the Environmental Justice League of Rhode Island; the Providence Children and Youth Cabinet in Providence; Thundermist Health Center in Woonsocket; Thundermist Health Center in West Warwick; the North Providence School Department; South County Hospital in Washington County; Women’s Resource Center in Newport; the Local Initiatives Support Corporation, or LISC, in Pawtucket and Central Falls; and the town of Bristol.
What the news release didn’t talk about in detail, as Novais explained to ConvergenceRI, is that the different lead organizations represented a diverse group, with different starting points – from a hospital system to a town, from specific city neighborhood to two neighboring cities – each collaboration with a different set of needs, each with a different kind of coalition.
And, as Novais emphasized, the story is still being written. “It’s not a story that we can tell on our own; it’s a story that we are writing together with the communities that we are working with.”
What we are doing, Novais continued, is this: “We are starting to write a new narrative, as we work together, because this is truly a partnership, that incorporates the pieces that we know, what the communities know, and now, how those communities are changing.”
As Gov. Gina Raimondo and her working group attempting to “reinvent” Medicaid begins its work, as the new statewide compact organized by Sen. Sheldon Whitehouse and R.I. Foundation President and CEO Neil Steinberg considers its next steps, they may want to take the time to sit down and talk with Novais, and listen carefully to what she has to say.
It’s a step that the Care Transformation Collaborative, formerly known as the R.I. Chronic Care Sustainability Initiative, or CSI-RI, is planning to take this week, as their leadership team has invited Novais to brief them on the plans for Health Equity Zones in Rhode Island, to explore potential points of convergence.
ConvergenceRI: Can you define what is meant by health as community? And, what is the importance of making these investments at the front end of the system, rather than dealing with people only after they become sick?
NOVAIS: This is a long journey. Let me put it this way. When we started trying to do this work, it meant shifting away from a medical model that is focusing on sick people.
For the past eight years, almost 10 years, we’ve been really trying to shift the way that we in public health approach those issues. And, how we can [achieve] better health outcomes from a population perspective.
It [begins with] a clear understanding that you cannot do this, unless you address the social and environmental determinants of health, the factors that we know affect health.
[A community’s health will not improve] if you don’t address the conditions of our neighborhoods, if you don’t address housing issues – not just housing being affordable, but housing that is safe, healthy housing; if you don’t address the lack of employment in the neighborhoods, and issues of self-sufficiency.
If you don’t have money to buy milk, how good is it going to be for me to tell you to do that? Or, that you need to buy fresh fruits and vegetables, if you don’t have them in your neighborhood?
How good is it for me to tell you that you and your children should exercise 30 minutes a day, if you don’t even feel safe to send your kids outside to play? Or, if it is safe to send them outside to play, that they don’t have any place to go?
We began three years ago. We invested in our first attempt of what I call a place-based approach, focusing our resources on defined geographic locations. What we called the Centers for Health, Equity and Wellness grants, the CHEW grants. And, we funded single organizations to do this work.
And, they developed wonderful strategies, in incredibly successful projects. Such as community gardens and the Lots of Hope program [in partnership with] the city of Providence, donating those abandoned lots to the community organizations. That was a step in the right direction.
At the same time, what we realized was that these projects were interventions. The services provided were very successful, but they were not truly changing the fabric of the community and the conditions in which people lived.
Three years later, we decided to say to these communities: we do not want to fund one organization; we want to fund an organization that is acting on behalf of a collaborative.
And, the collaborative needs to be truly defined by the folks, the residents, the groups that are part of your collaborative.
You all need to agree that you are working toward a single vision; that vision needs to be determined not by a single organization, but by the collaborative.
You need to do a local assessment of what are the needs of the residents, and to collect information that is going to inform that vision, that’s going to inform the development of the community’s local priorities, [shaping] that into a plan of action. And, then, we will fund the implementation of that plan of action.
ConvergenceRI: It’s a phased approach.
NOVAIS: Yes, a phased approach. In the first year, we are saying to those communities: define the boundaries of your [Health Equity] Zone. I’m not going to define it for you.
Some people are defining it as a specific neighborhood. For instance, Olneyville Housing is the lead organization for one collaborative. They have defined [the Health Equity Zone] as a line drawn around Olneyville.
We are saying: define that; build your collaborative.
We are going to give you six months funding, for you to engage with partners, to bring them together, to take the time to get to know each other, to understand the different agendas, and to start to work together toward assessing your community in terms of strengths, in terms of assets, in terms of gaps, in terms of needs.
Then, collectively, once you complete that process, finding out what each of you brings to the table, you are going to define the priorities.
Our goal at the end of year one is that we will have the collaborations well established, that the needs assessment [will be] done, and that there is the beginning of identification of priorities and the plan of action.
And so, funding in years two and three will be to support the implementation of the plan of action.
ConvergenceRI: Your expectation is that the collaborative will set the priorities, and not the priorities of the lead organization?
NOVAIS: Yes, because we are not funding just one organization, but a collaborative. While the money is going to a backbone organization, the expectation is that it will support activities and strategies across all members of the collaborative, so that those organizations are also funded.
They all will own a piece of the implementation.
We are also expecting, that while the groups are supporting a piece of the implementation, the [members of the collaborative] will be incorporating the new priorities into what they were already doing.
So, that [the work] is sustainable after our funding disappears, because it becomes more integrated.
That’s a broad overview of how we are approaching it.
ConvergenceRI: Can you talk about the different approaches? The different starting points, for the collaboratives?
NOVAIS: We have a variety of models for Health Equity Zones. One is them is a hospital system, South County Hospital. Louis Giancola, [the president and CEO], is being very creative in his approach to public health. South County put a group together to create a collaborative for Washington County.
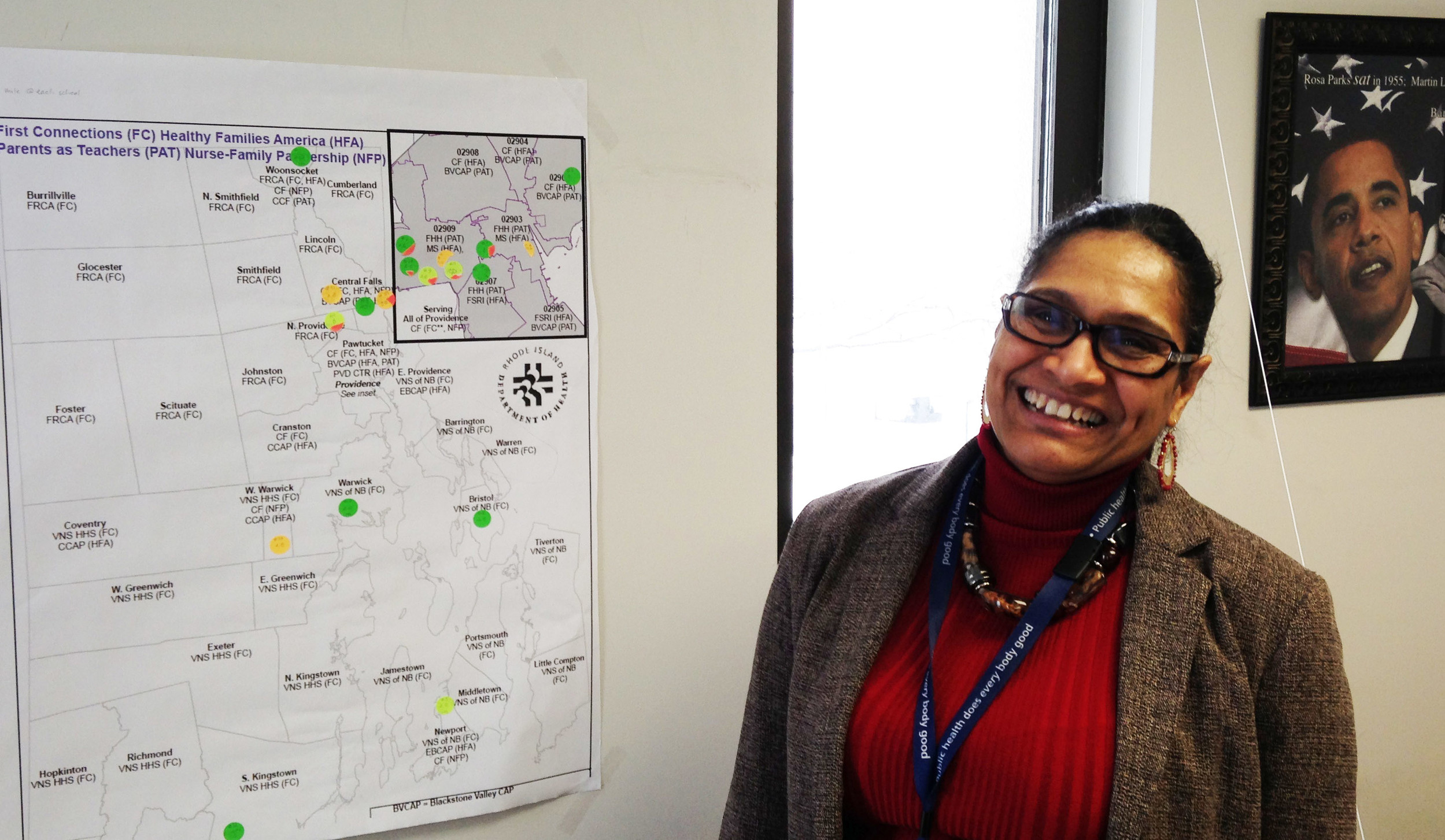
ConvergenceRI: I see two different maps on your wall. What do they represent?
NOVAIS: One is a Providence map, and then I also have a statewide map.
We wanted to have a Health Equity Zone, at a minimum, one in each county, and we have done that.
We also have a number in Providence County; we have funded Health Equity Zones in Providence, in Pawtucket, in Central Falls and in North Providence.
ConvergenceRI: Do you believe that there is enough money in the current health care delivery system to fund future community health investments?
NOVAIS: Yes, I absolutely agree with that. I don’t think that the issue is a lack of funding. I think the issue is how funding is being allocated throughout the system.
The Health Equity Zones don’t exist within the health care system. They ought to be seen as an integral part of the continuum of care.
We have South County Hospital; we also have Thunudermist, [a community health center]. Thundermist is applying as the backbone organization in Woonsocket and West Warwick, but they are two different collaboratives and two different approaches.
This shows the integration between clinical and community, the need for clinical and community linkage, and how those two approaches connect.
We are also not looking at the Health Equity Zones and these kinds of investment in isolation.
I have asked all of our programs in the Department of Health: what are the other investments we have made, for example, in Woonsocket?
We have made a huge investment with family visiting, for example. We are requiring our teams to participate in every Health Equity Zone that have local implementation teams for home visiting, to bring those efforts together, to engage with them, and to make sure we leverage that work. And, to make sure that those families that we served in our home visiting programs are part of the needs assessment and the solutions.
It links to all the other investments that we are doing.
ConvergenceRI: Can you talk about the differences in the way that population health and health outcomes are being defined?
NOVAIS: There are two ways to look at population health. You can define population health by looking at a target, a specific population, meaning those that I serve. If you are a Medicaid agency, population health traditionally will be the population that you serve under the Medicaid program.
If you are an Accountable Care Organization, you define population health as the patients you serve, with them being active or not, and that’s the traditional approach.
Or, you can take that definition one step further, and think about population health and the population that you serve as the population that surrounds where you are – the larger, broader community that you are interfacing with.
If you do it that way, it opens the door for a better understanding of the continuum of services that any delivery system needs to have.
I don’t like to talk about health care delivery systems; I like to talk about health delivery systems. It clearly identifies the need for community engagement.
I’m happy to say, I think that some of the folks understand that. But it’s hard to operationalize that notion.
[The R.I. Chronic Care Sustainability Initiative], for example, very clearly understands what the connections are. In fact, I’m doing a presentation to the CSI steering committee leadership team next week about the Health Equity Zones.
I believe the conversation is happening because they realize that there is a win-win in making sure that we establish connections.
They have established community health teams; those community health teams are similar to what will be created as part of Health Equity Zone.
We are talking about community health workers. Aren’t those the same? Whether you talk about community health workers, navigantes, peer resource specialists?
Wouldn’t it be great if you had a system in Rhode Island that had an agreed upon core set of competencies?
You could create a career and a career-ladder for that kind of specialty. And, it becomes an economic development strategy.
We are working with a group that includes Medicaid, the Department of Human Services, the Department of Behavioral Healthcare, Developmental Disabilities and Hospitals, the R.I Parent Action Network, Maternal and Child Health. We started it as a quality improvement project.
The goal, viewing it from a workforce development [perspective], is to see what core set of competencies we are going to agree upon. To develop a list, identify a trainer, and get people to be reimbursable. That’s economic development.
ConvergenceRI: Can you describe the different approaches being taken by the Health Equity Zones? For instance, talk about the Health Equity Zone being funded through LISC in Central Falls and Pawtucket. Who is involved?
NOVAIS: Every single one of the Health Equity Zones are very different. Every one has developed a group that is linked to the kind of proposal they are doing.
For example, with the LISC proposal you mentioned, I have Progreso Latino, the Pawtucket Central Falls Development Corporation, the Rhode Island Public Health Institute [they are helping with the evaluation and assessment], the city of Central Falls and its office of Planning and Economic Development, the Central Falls Housing Authority, the Central Falls school district, the city of Pawtucket and its department of Planning and Development, the Pawtucket Housing Authority, Memorial Hospital of Rhode Island, Blackstone Valley Community Health Care, the Rhode Island Coalition against Domestic Violence, the Providence Center, Blackstone Valley Community Action, and the Children’s Lead Action Project.
It’s very diverse group of partners, reflective of the kind of work that they are going to be doing. They came in with a very comprehensive proposal with very specific, already identified priorities, [based upon] existing assessments that have been done for Central Falls and Pawtucket.
ConvergenceRI: How does that compare with, say, Bristol?
NOVAIS: The town of Bristol is one of our awardees for Health Equity Zones. They recognized, from the get-go, that they are new to this work, and that they were not sure how to do it.
But, they recognized, as a first step, they needed to bring the people of Bristol together, the residents of Bristol, to help them define what the Health Equity Zone was going to address.
In fact, their proposal was modest, in the sense that they asked us for funding, at this moment only for year one, to help build their collaborative, and to bring on some consultants to help them create the collaborations and identify their collective visions, and start their assessment of needs.
They told us, we don’t have a work plan; we don’t have a plan of action.
And, that is perfectly appropriate.
You can have a very tiny application from the town of Bristol, saying that it needs to bring folks together as a first step, so we can start to understand what to do, how make an assessment of needs, and I need help in year one to do that.
Or, you can have a very comprehensive application, like the one from the Olneyville Corporation, which has been working collaboratively to focus on a place for many years, which was one of our CHEW grantees, and it’s building on that work to do the next phase of implementation of a comprehensive package that includes housing and job training, with all of those elements focused on the determinants of health.
ConvergenceRI: That is a big spread, between plans for the Health Equity Zones in Bristol and in Pawtucket and Central Falls.
NOVAIS: That’s the kind of spread that we have. In North Providence, for example, also very municipality driven, the lead applicant was the North Providence School Department.
They are focusing on the Marieville area as a pilot, because they said, we’re not sure how to do this. So, we want to start small, we want to focus initially on Marieville, and then we want to expand to North Providence.
ConvergenceRI: Some 20 years ago, United Way of Rhode Island worked to help develop a series of coalitions known as Child Opportunity Zones. They may still exist, but I have no idea what they are doing and how they are doing, or even if they still have a reserve of funds. Did you ever hear about COZies, as they were called?
NOVAIS: I do not know what they are doing or not doing, or if they exist or don’t exist.
I think the notion may have been probably similar, in terms of focusing on areas with disparate health and educational outcomes for children and try to address them.
I think, perhaps, the difference may have been in the approach, in that the solution that was proposed may have been more focused on services.
Meaning, [it was focused on] rescuing people. You keep rescuing people, you keep rescuing people. While it was an improvement, it focused on an area of bad outcomes, the solution was seen as services to rescue folks in trouble.
What we are saying with the Health Equity Zones is different. Unless you work in the community, addressing the conditions that are creating that burden of disease, you are always going to be rescuing people. And, there is no money, not enough money, to rescue people indefinitely.
If you start to diminish the conditions that led to the poor outcomes, then you are going to be more successful.
ConvergenceRI: How are you going to tell your story? Has any thought been given to how you want to tell the story of what you’re doing?
NOVAIS: I want to tell the story, but it’s not a story we can tell on our own. It’s a story we are writing together with the communities that we are working with.
There are parts of the story that I know – that the state knows. That’s the part of the story from our data, from our assessments, with identifying health disparities.
There is a part of story that the community knows; they know what’s happening at their local level. They need that story to be told, too.
As we work together, because this is truly a partnership between the state and those local communities, we are starting a new narrative.
At the end of three years, we want to tell that story, we want it to be a big story, we will have chapters to tell as we go along.
On May 7, we’re going to have a Health Equity summit. We’re going to bring all of our CHEW grantees for the past three years together, along with the new grantees in the Health Equity Zone program, along with other national and local experts, to have a conversation.
The focus will be on the indicators that we want to see changed, what the CHEW programs were able to achieve in the past three years – where they were successful, and what were the lessons learned – so we can start creating that new narrative.
And, I hope that ConvergenceRI can help us tell that story.
ConvergenceRI: How do you think that the narrative of health care in the state of Rhode Island needs to change?
NOVAIS: I don’t have an answer to that. I think it’s more than just when people are connected. I think it’s when state agencies, key decision makers, and local agencies are connected. You cannot transform and change conditions at the local level, or social and environmental conditions at the state level, if we are not connected, both from a state agency’s perspective and a local agency’s perspective.
ConvergenceRI: Any plans to run for elected office?
NOVAIS: [laughter] I’m not a politician; I am a public health servant.
I truly believe that people, if they take the time to build relationships, if agencies take the time to understand how connected they already are, and to recognize the things that they share, [people and communities will prosper].
If we take the time to do that, it makes it easier.
I go back to eight years ago, when they asked me to lead this division, which was created from three separate divisions, one focused on maternal and child health, one focused on chronic diseases, and one focused on environmental health.
They were different divisions, with different lingos and language, and different approaches. My challenge was to figure out how to bring them together.
I really took the time to try and understand what was common between [the divisions], not just for me, but for them, so that they could understand what were the linkages that already existed. And, maybe they were using different language [to describe their work], but they were doing the same things.
Social and environmental determinants, for example, were words that the chronic disease division was using. I said to them: environmental health has been addressing social and environmental determinants for a long time; they just don’t call it that way.
That’s what they’re doing, when the lead program is doing assessments and testing. They are impacting our asthma program in chronic diseases; so how can we make those two divisions work better together?
When we have our diabetes program [in the chronic disease division] addressing gestational diabetes, they are addressing maternal and child health issues. By recognizing that, by taking the time, they could understand what the linkages were.
With Health Equity Zones, I am hopeful that, by doing it is this way, by giving these communities the time to create the collaborative, to understand the relationships, they will be able to shape a common vision and work collectively toward the same goal.




