
Trouble ahead, trouble behind
Who is going to be driving the future public health train?
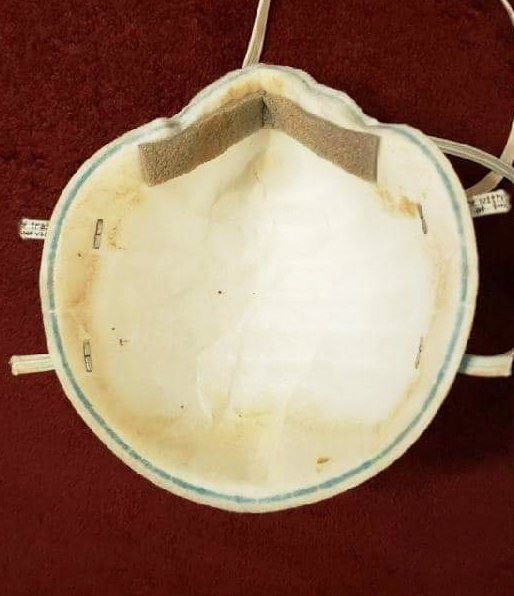
“This is an actual ‘decontaminated’ N95 mask that Albany Medical Center gave a nurse to use,” as tweeted out on Friday, Oct. 23, by Pat Kane.
In response, Dr. Megan Ranney, an emergency room physician in Rhode Island, responded: “I have no words for how wrong this is, and how angry it makes me.”
Ranney, who has set up a nonprofit, get usppe.org, continued: “I dare you to suggest that this mask still has structural integrity and can protect this nurse. We are the United States. Our frontline workers deserve better than this.”
The reality is that as Rhode Island and the nation enters a new surge of coronavirus cases, hospitalizations and deaths, the lack of personal protection equipment, or PPE, continues to be a major problem, threatening the health and well-being of nurses, doctors and patients.
I had that phrase repeated to me by at least five different people, from numerous walks of life, to which I asked them: Have you ever met Bernie Sanders? No, they responded, but it seems like you could sit down and have a beer with him, they repeated.
The problem was, I told them, it wasn’t true: I had dealt with Sanders on a number of different occasions. And, while I can admire his tenacious political advocacy, he was never, in my experience, an “easy” person to deal with. In fact, Sanders had a reputation of being difficult, an observation shared by many of my friends who live in Vermont and who have been active in politics for the last four decades.
No matter. There was a major propaganda effort, supported by Fox News, to portray Sanders as a “likeable” guy – the one you could get a beer with – and to disparage Clinton as somehow less likeable. To a large extent, the false narrative worked.
When it comes to health care, we are often confronted with a false narrative, carefully sculpted in advertising, mailers and billboards. The problem, however, is that for those who must confront the daily struggles to advocate for themselves or their families through the maze of health care delivery in this time of pandemic, the direct experience contradicts the positive corporate messaging.
The coronavirus pandemic has torn away the façade of the benefits of corporate health care. Potemkin villages built on advertising slogans will not cover up more than 220,000 dead in the U.S. – and counting.
Editor’s Note: President Trump claims that we have “rounded the corner” when it comes to the coronavirus pandemic, but Johns Hopkins University reported 83,757 new cases and 943 new deaths on Friday, Oct. 23, the highest number of new cases reported in a single day since the pandemic began appearing in late February in the U.S..
Worse, the positive rates in states across the nation keep rising: On Saturday, Oct. 24, the latest data from the Johns Hopkins Coronavirus Resource Center showed South Dakota at 38.5 percent; Idaho at 34.3 percent; Wyoming at 27.6 percent; Iowa at 23 percent; Alabama at 21.7 percent; Nebraska at 19.5 percent; and Utah at 17.2 percent – all states run by Republican governors.
Here in Rhode Island, the rise in new cases hit an all-time peak – 449 new cases of COVID-19 were identified on Thursday, Oct. 22, according to Gov. Gina Raimondo, resulting in a 3.2 percent positive rate, even as the state crossed the 1 million tests performed threshold.
At the Wyatt federal detention center in Central Falls, the number of prisoners with COVID-19 had reached 124 as of Friday, Oct. 23, nearly one-quarter of the facility's 545 detainees, according to state Rep. Jason Knight.
Translated, the trend lines keep moving in the wrong direction, big time. Containing the spread of the virus is the urgent task at hand as the nation moves into the colder, winter months. But it is equally important to keep our eyes on the prize, asking questions about what lessons can be learned from our experiences with the coronavirus pandemic – and how we need to reshape our thinking about the delivery of health care services.
Dr. Peter Simon, retired epidemiologist and pediatrician, offers up some questions to consider as part of the learning curve.
PROVIDENCE – Those with “power” and “money” have determined the shape of our health system. Without a shared understanding of the burden of disease and threats to the health of the people of Rhode Island – and their experiences seeking care in the present time, we may not see much changing for the good for us all in the future, following the coronavirus pandemic.
What we know and what we need to know
Off the coast of Greece, there are several island communities where residents routinely experience good health into their 10th decade. Researchers for decades have set up shop on these islands to observe and measure the patterns of living to see what are the elements that contribute to these healthy outcomes.
I know there are five determinants often cited from this work: genetics, behavior, environmental and physical influences, medical care and social factors.
How many of these five interconnected determinants have been discussed as part of the future long-term planning for health in Rhode Island? For instance, what are the projected health costs for rebuilding the Route 6/10 Connector in terms of future chronic disease burdens on the communities surrounding the highway?
Longitudinal design
When looking for the causes of risk, disease or any adverse outcome, I was taught by Dr. George Comsock, my professor of Epidemiology at Johns Hopkins University School of Hygiene and Public Health, many research designs are available but none can compare to longitudinal design.
One study that meets such criteria that many will recognize is the Framingham Heart Study. Can anyone name another similar study in the U.S.? Or, here in Rhode Island? The ongoing research by Professor Anna Aizer, chair of the Economics Department at Brown University, looking at the longitudinal outcomes for lead-poisoned children in Providence, is one.
Much of the evidence based on causality – the science of looking at observed relationships between cause and effect – can often be flawed by a misuse of cross-sectional research design as well as the misunderstanding of the different types of risk.
The use of data as evidence
I wonder: what kind of “evidence” is being developed to look at efforts now underway to determine future health care delivery in Rhode Island?
Now, don’t get me wrong. I think what the forces behind the Rhode Island Foundation effort to develop plans for health, education and racial equity are wonderful.
I am just wondering a bit how their findings and recommendations might change and evolve if their deliberations had occurred after the current pandemic.
My questions are: What have we learned about ourselves, and the strengths, weaknesses and opportunities for our state’s health system – for both preventive, acute and long-term medical care services?
Would the priorities for investment in our community health and well-being be different today, with what we have seen from the epidemiologic examination of infections, hospitalizations and deaths from COVID-19?
Institutions with the power and the money often dominate a planning process, keeping it from being balanced and community-driven, in my experience.
Unless people come together and establish a common understanding of what health is and where it comes from, recommendations for future investment will be skewed toward the institutional interests of the most powerful and best financed, in my experience.
The vision for what we want in the future needs to be informed by real experiences of all members of the community, not just those now in paid government roles, those running large hospitals, and administrators of schools of Medicine.
As I write this, what keeps popping into my head are the memories of what happened to early efforts around “regional planning” to support healthy people, when the process was disrupted by those who told us told us that the government was the problem, not the solution.
“Regional planning” became a victim of those on the right who sought to eliminate comprehensive health planning that restricted those more interested in preserving their institutions or commercial gain.
My recommendations
First, I believe there needs to be a bright light, making transparent how the money from Brown University, Lifespan and Care New England – and other corporate stakeholders such as CVS and commercial insurers – will flow into the “planning and design” of the process for consolidation of our major health services institutions.
How will these large and politically connected entities invest in ways that serve the interest of the under-represented? Is there a way to follow the money?
Second, will the Rhode Island Foundation commission a “follow-up” report to its stakeholders, analyzing the lessons learned from the coronavirus pandemic, as a way to influence future deliberations around what will make Rhode Island the healthiest state in the nation?
Third, what research and studies are being commissioned now to look at the longitudinal outcomes of health during the coronavirus pandemic in Rhode Island, tied to neighborhoods and minorities?
Dr. Peter Simon is a frequent contributor to ConvergenceRI.




